







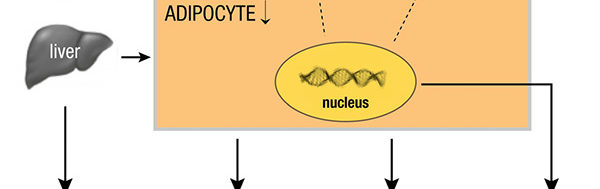
Molti studi clinici hanno dimostrato che il testosterone, e gli androgeni in generale, possiede spiccati effetti anti-infiammatori. Tale effetto si esplica prevalentemente inibendo la formazione del grasso corporea, in particolare dell’adipocita che è la sorgente principale delle citokine infiammatorie. In particolare il testosterone inibisce la formazione di interleuchine (IL-6, IL-1, TNF-α). In soggetti con bassi livelli di testosterone circolante la componente infiammatoria è aumentata, mentre la terapia con testosterone la inibisce.
Low plasma testosterone (T) levels correlated with metabolic syndrome, cardiovascular diseases, and
increased mortality risk. T exerts a significant effect on the regulation of adipose tissue accumulation,
and in the glucose and lipids metabolism. Adipocytes are the primary source of the most important
adipokines responsible for inflammation and chronic diseases. This review aims to analyze the possible
effect of T on the regulation of the proinflammatory cytokines secretion.
A systematic literature search on MEDLINE, Google Scholar, and Cochrane using the combination of
the following keywords: “testosterone” with “inflammation,” “cytokines,” “adiponectin, CRP, IL-1B, IL-
6, TNFa, leptin” was conducted. Sixteen articles related to the effect of low T level and 18 to the effect of
T therapy on proinflammatory cytokine were found.
T exerts a significant inhibitory effect on adipose tissue formation and the expression of various
adipocytokines, such as leptin, TNF-a, IL-6, IL-1, and is positively correlated with adiponectin level,
whereas a low T level is correlated with increased expression of markers of inflammation. Further
studies are necessary to investigate the role of T, integrated with weight loss and physical activity, on its
action on the mechanisms of production and regulation of proinflammatory cytokines.
Copyright © 2019 Endocrine Society
This article has been published under the terms of the Creative Commons Attribution Non-
Commercial, No-Derivatives License (CC BY-NC-ND; https://creativecommons.org/licenses/by-ncnd/
4.0/).
Freeform/Key Words: testosterone, inflammation, cytokines, adipokines, adiponectin, IL-6
The development and progression of chronic diseases are correlated with low T level and
inflammatory biomarkers, but their mechanisms remain poorly understood. T deficiency
(also known as hypogonadism) in older men has been associated with metabolic syndrome [1],
neurodegeneration [2], and increased risk of cardiovascular diseases (CVDs) and all-cause
mortality [3] independently of other numerous risk factors [4, 5]. Similar observations were
reported in young men [6]. Before any concurrent manifestations of CVD or other systemic
diseases, low T level is correlated with elevated C-reactive protein (CRP) level [7], macrophage
inflammatory protein 1-a,macrophage inflammatory protein 1-b, and TNF-a in young
and older men [8]. CRP is a sensitive marker of inflammation produced by liver [9] and is
correlated with coronary heart disease and deaths from other causes [7].
An inflammatory status due to proinflammatory cytokines is particularly evident in the
elderly [10], and in patients with low T levels and obesity [11]. Furthermore, adipokines
mediate insulin resistance [12] and the principal adipokines involved are adiponectin, leptin,
resistin, visfatin, chemerin, TNF-a, IL-1, IL-6, IL-8, IL-10, plasminogen activator inhibitor-1,
monocyte chemoattractant protein-1 (MCP-1), and retinol binding protein-4 (RBP-4) [13].
Higher levels of proinflammatory cytokine play a crucial role in the development of CVD [14],
and T therapy provides beneficial effects on the pathophysiological markers and clinical
symptoms of coronary heart disease [15].
Furthermore, adipokines are involved in the development and progression of cancer
[16]. The etiology of elevated inflammatory markers remains incompletely defined [17],
Abbreviations: BMI, body mass index; CRP, C-reactive protein; CVD, cardiovascular disease; ER, estrogen receptor; HMW, high
molecular weight; MCP-1, monocyte chemoattractant protein; OPG, osteoprotegerin; PCOS, polycystic ovary syndrome; T,
testosterone.
but nutrition and physical inactivity also exert a primary role. Little is known about if and
how sex steroid hormone and inflammation pathways may interact to influence the
aging process or the development and progression of chronic diseases, including CVD
and prostate cancer, in men. This study aims to evaluate the effect of T on proinflammatory
cytokines.
1. Methods
A systematic literature search was performed using PubMed, Google Scholar, and Cochrane
using the combination of the following keywords: “testosterone” and “inflammation,” “cytokines,”
“adiponectin,” “CRP,” “IL-1B, IL-6, TNFa, leptin.” All cross-sectional and longitudinal
trials evaluating the incidence of low T in men with moderate to severe inflammation
were included. Furthermore, clinical studies that investigated the effect of T administration
on inflammatory markers were also considered.
2. Results
Out of 824 retrieved articles, 35 were included in the analysis and had been divided into two
groups: one group includes 17 studies evaluating the incidence of inflammatory diseases in
men with low T level enrolling 14,658 patients with a mean age of 59.96 12.8 years (Table 1).
The other group includes 18 studies that evaluated the effect of T therapy on plasma level of
inflammatory markers enrolling 1654 patients with a mean age of 56.4615.6 years (Table 2).
Among the first group, only one study did not find any correlation between T level and CRP,
but this study was conducted on healthy middle-aged men, whereas all the other studies
found a significant negative correlation between T level and inflammatory markers. Among
the studies evaluating the effect of T therapy on proinflammatory markers, six studies found
no effect.
3. Discussion
Low T levels in men were significantly associated with high level of inflammatory markers in
different clinical conditions such as obesity [18], metabolic syndrome [19, 22, 32], heart failure
[33], healthy elderly population [20, 22, 27, 28, 30], carotid atherosclerosis [23], hypogonadism
[8], urologic symptoms [26], type 2 diabetes [29], primary care center [34] and are
summarized in Table 1. In all studies, a negative correlation was found between low T levels
and CRP, whereas only a few studies explored IL-6 [18, 30, 33] and TNF-a [8, 33]. Haring et al.
[24] found a negative correlation between sex steroids plasma level in men with markers of
inflammation. Bhatia et al. [29] showed that low T was inversely correlated with CRP and
may contribute to mild anemia. Maggio et al. [30] found that T level was inversely correlated
with IL-6r [35]. An extensive epidemiological study revealed that men with low T level had a
higher incidence of obesity, metabolic syndrome, cancer, and acute inflammation [34]. Only a
few studies had adjusted the data for other sex hormones [21, 35]. In elderly men, the reduced
levels of T were correlated with the incidence of metabolic syndrome, insulin resistance, and
inflammation evidencing that high CRP levels can be considered independent predictors of
metabolic syndrome [19, 22]. Some studies that evaluated the correlation of CPR with low T
level did not adjust for other confounders such as smoking and obesity [22, 23, 25, 27, 34]. A
few epidemiologic studies did not find any consistent correlation between sex steroid hormones
and inflammatory biomarkers in men [30–32]. Others found a negative correlation
between the level of androgens with inflammatory markers [21, 25–28].
The majority of the studies found an evident protecting effect of T against inflammation
independently of the clinical condition. However, it is difficult to draw a global evaluation
because only a few studies have detected more than one cytokine in addition to CRP [8, 18………
